






SHARE THIS ARTICLE:
NH – Senate Health & Human Services Comm.
March 29, 2005
Testimony of Pat Smith, Lyme Disease Association, to the New Hampshire Senate Health & Human Services Committee
I want to thank Senator Kenney for introducing the bill and for requesting LDA testimony and the Committee for their time and consideration of the bill.
Lyme is the most prevalent vector-borne disease (insect & tick-borne) in the US and the most prevalent vector-borne bacterial disease in the world.(1) Different ticks are now carrying Lyme or a Lyme-like illness called STARI, southern tick associated rash illness.(2) The range of these ticks appears to be spreading with the lone star, which 15-20 years ago only was found far north as central New Jersey, now found as far north as Maine.
With one tick bite, you may contract one or more tick-borne diseases (TBD) some of which include Lyme, babesiosis, anaplasmosis, Ehrlichiosis, bartonella, tick paralysis, STARI, and tularemia, complicating an already difficult diagnostic process and treatment regimen.
From poppy-seed to sesame seed size, deer ticks, the main Lyme disease tick vector, can transmit bacteria that can wreak untold havoc on the infected individual and family. Dozens of doctors, years of treatment, lost income, and piles of unpaid medical bills are only part of the scenario; the lack of emphasis placed on Lyme disease by many in the medical and governmental communities is another. To help address that education issue, LDA and Columbia University will jointly present LDA’s 6th Lyme & Other Tick-borne Diseases conference this year in Philadelphia in October for physicians and health care providers and the public.
Lyme disease is serious. The bacterium can enter the central nervous system within hours of a tick bite (3) ; it can hide in your cells: a Sept 2004 article in The American Journal of Pathology presents research that confirms that the bacterium is able to hide in certain places in the body (skin & Joints) and evade the immune system. Also, it can mutate, change into forms unrecognizable to conventional antibiotics, and can go in and kill cells that are supposed to kill it (see photo at end). It can even perform a Star Wars maneuver: it can enter your cell and come out cloaked in the body’s own membrane, (4) unrecognized as the enemy it is. It can cross the placenta, it can cause birth defects and death of the fetus, and it can kill those infected.
Lyme can attack every system in the body and is called the great imitator since it can mimic many other conditions including MS, ALS, CFS, FM, lupus, Parkinson’s, Alzheimer’s, and even autism.
Research has shown that the bacteria can survive in blood under blood banking conditions, (5) and the Red Cross has changed blood donor guidelines now prohibiting those diagnosed with chronic Lyme disease from giving blood.
Our children are at the greatest risk of acquiring the disease, and they may spend years out of school due to effects of the disease. Columbia University research has demonstrated a 22 pt. IQ drop in a Lyme patient, reversed with treatment. (6)
LDA and its CT affiliate Time for Lyme are partnering with Columbia University to open an endowed research center there for studying chronic Lyme disease. LDA is also supporting research mapping genomes of different strains of the Lyme bacteria. The first phase of that research was published in The Proceedings of the National Academy of Science, Sept 2004, initially funded by LDA and later joined by NIH funding. That research showed that different strains of Borrelia can quickly exchange genetic material among themselves enabling them to better survive and confound testing procedures.
Unfortunately, the monies our organizations can provide are relatively small, but research requires a concrete monetary commitment commensurate with Lyme’s status. Based on Centers for Disease Control reported case numbers which it says are only 10% of cases that meet its criteria, about 220-240,000 new cases of Lyme disease develop each year, and research studies have shown a prevalence of persistence of 34-62% of Lyme patients. (7)
The Society of Actuaries conducted a study of over 500 patients and found the average reported costs of the difficult cases was over $60,0000 patient. (8) A CDC 1992 NJ school district study showed median total direct medical costs at $48,000/child in a study where the mean was 103 days out of school, and the mean duration of illness was 753 days. (9)
Yet the government, particularly the CDC, is expending relatively small amounts of monies to research the disease. In 2003, LDA took a team of 14 to Washington DC to present to the Health & Human Services office of Tommy Thompson the issues surrounding Lyme disease─one issue the lack of funding. The CDC, for example, from 99-2003, shows its LD funding was constant at $7 million, totaling $35 million over the period, while West Nile went from $0 to $38 million, totaling $119 million over the same period.
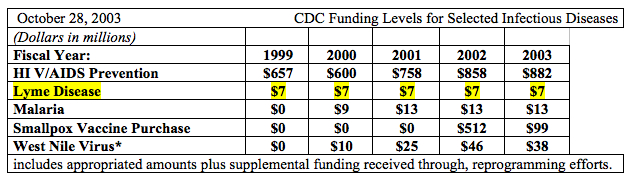
Resolutions such as your can make a difference in the funding area. Note the reference to increased public/political attention to disease resulting in separate accounting below from the CDC:
In addition, separately tracking diseases in the accounting system usually occurs when: new money is appropriated from Congress for the first time for a specific disease; when there is an outbreak of a new disease; and when there is increased public/political attention to a disease. (10)
Remember that Lyme disease does not discriminate, nor does it confer immunity. Risky behavior includes walking the dog, jogging, or playing in the backyard. The only thing standing between you, your family, and Lyme disease may be the power of new government research monies to unlock the secrets of Borrelia burgdorferi, a bacterium causing Lyme disease.

A scanning electron microscope image of Borrelia burgdorferi penetrating a human B cell at a magnification of ~13,700
Courtesy: David Dorward, PhD Rocky Mountain Labs MT
I will be available for speaker phone questions if necessary after 10am Tuesday March 30 at 732 938 4834.
End Notes:
1CDC website
2CDC website
3Steere A et al Bennett’s Principles & Practices of infectious Diseases 1995
4David Dorward, PhD, NIH Rocky Mt Labs
5Johnson SE et al J Infec Dis 1990 Aug;162(2):557-9
6Fallon B et al The Psychiatric Clinics of NA Sept. 98
7Shadick NA et al Annals of Internal Med. 94. Asch ES et al Rheumatol. 94.
8Vanderhoof et al Contingincies, 93.
9CDC & NJDOH field study 1992 unpub. Presented at Congressional Lyme Forum Wall NJ 1992
10Information presented by LDA Team to HHS in DC meeting, Nov. 2003